Problems That Don’t Have to Be

Problems That
Don’t Have to Be.
34,186 people watched a poorly made video filmed at 4am after an exhausting day, month, and two years. This is the full story — written Wednesday, labs today, rest of the week unknown.
How we got here.
I didn’t plan to start a blog series. It was nowhere on the list. But here we are — because of a video I posted at 4am, raw and unpolished, made in the middle of chaos — and 34,186 people watched it.
My wife Melody couldn’t care less about metrics. Reach, growth, algorithm — not her world. I handle that, for my own brands and for clients. But that number? She watched it climb. 21k. 22.5k. 31k. In a week. Getting up some mornings and asking before anything else — what’s it up to now? You could see the joy on her face. In a week that had very little of it.
My hope is that this post does the same thing. That you watching, reading, sharing — brings her that again. And beyond that: imagine what 34,000 people coming together with one voice could actually do. Real change. Meaningful change. The kind that makes systems work for patients instead of around them. That’s what this series is for. Not sympathy. Action.
“You responded. So keep responding. Watch. Share. Come back. Together we are loud enough to bring healthcare back to the patient.”
That’s why this series exists. Not to perform grief. Not to beg. To pull back the curtain — and to advocate for every patient sitting in a waiting room right now wondering why a system this expensive works this poorly. If you’ve been there, you know. If you haven’t — you’re about to.
Meet Melody.
Melody’s health journey started before most people’s adult lives do. She was diagnosed with a rare autoimmune disease — discovered accidentally, by the grace of God — that was destroying her liver. She received a liver transplant in her late teens.
The transplant brought its own consequences. A particular assault on her cardiovascular system. No blood flow to one kidney. Renal stenosis. A steady decline of the other. Complicated by providers with cookie-cutter solutions and bright ideas, her remaining kidney failed completely.
She was evaluated for a kidney transplant. Denied by one provider. Approved by another — except not really approved. She was approved and immediately put on hold. Always one more form. One more test. One more specialist to verify. A circle that never closed. Volunteers came forward to donate. The system that approved her never received the submissions. Three applications to reach the step the previous two said was next.
2025 brought six hospitalizations. Continuous pneumonia — and not until the end of the year did any of her providers refer her to a pulmonologist. Like her kidney failure, the pattern is consistent: manage what’s visible, until it’s too late to do much about what wasn’t.
In March, a bone marrow aspiration confirmed MDS — Myelodysplastic Syndrome, SF3B1-mutated subtype. A rare blood cancer presenting as severe anemia. We got those results in October. Seven months later. After a new oncologist had to demand them from the previous one — who had kept Melody waiting over an hour on a dialysis day, in a weakened state, then simply left.
Getting that bone marrow aspiration in the first place was its own fight. The hospital wanted to discharge her and do it outpatient. I pushed back. The decline had been building since fall 2024 — failure after failure by the same system that demands so much compliance from her. She will tell you, and has told every provider who will listen: they don’t hear her. They look at the labs. They don’t look at the patient. Getting them to order the test that confirmed her cancer required someone in that room who wouldn’t accept “the labs look okay” as a complete answer. That is the theme of this entire series. Everything — every single thing — is a fight to get them to treat the actual person in the bed.
The Monday after discharge, I called the oncologist’s office. I was told — with a chuckle — “The doctor said if there was a concern, she would call you.” MDS. Cancer. Apparently not worth a call.
Today.
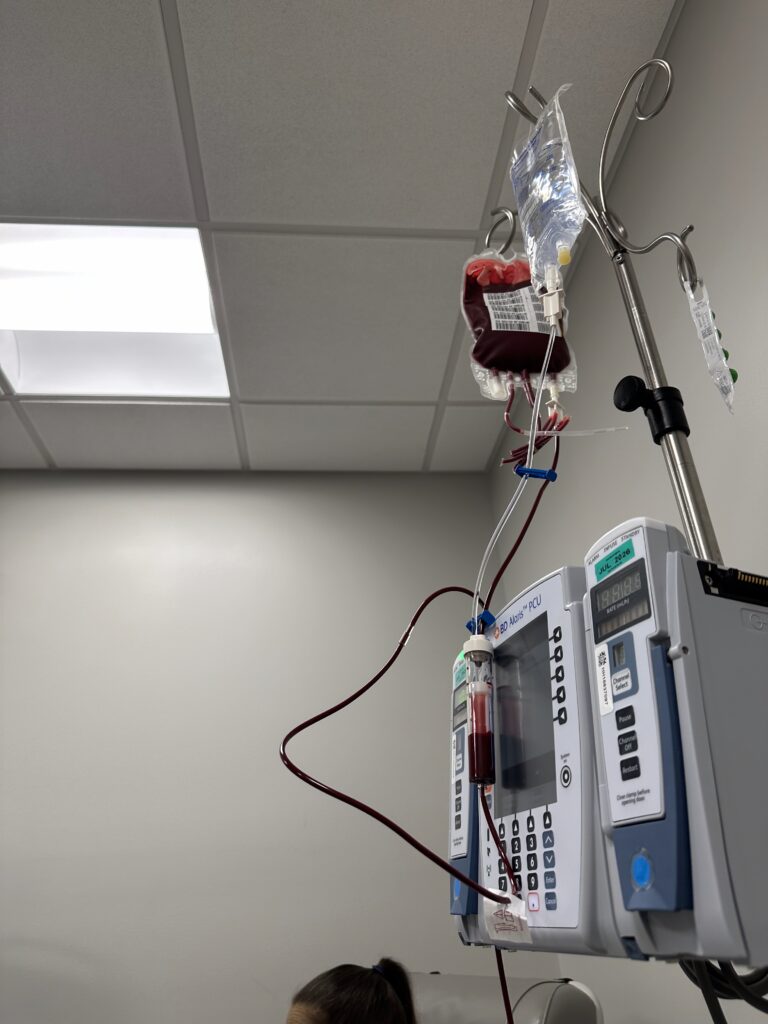
Today, Melody is blood transfusion dependent. She needs one every week. Sometimes twice. This is not temporary. It is increasing in frequency. It is entirely predictable — which makes what follows even harder to explain.
Her oncologist set the floor at 8. Below 8 g/dL hemoglobin — she needs a transfusion. To schedule one at the infusion center adjacent to her oncologist’s office: typically two days. Last time, three — which is why she ended up in the ED the week before this story.
The hospital disagrees with the floor of 8. That disagreement has consequences. We’ll get to those.
The week it happened.
Her mother’s birthday fell on a dialysis day. Dialysis is scheduled months out — immovable. Birthdays don’t move either. So they planned the celebration for the next day instead. That’s the kind of thing that doesn’t make it into the discharge notes. The quiet sacrifices patients and families make around a schedule that belongs to the system, not to them.
Monday’s labs showed her hemoglobin at 8.2 — a number it rarely reaches. Oncology said no transfusion needed. But she was symptomatic: labored breathing, low energy, that specific ache in her legs she knows by name. She knew. Tuesday was dialysis. She didn’t want to go back to the lab.
Wednesday — labs with her mother. Birthday celebration day. The oncologist called urgently: go to the ED now.
Here’s what the labs actually showed across the week:
- May 188.2 g/dL — oncology says no transfusion needed
- May 20 AM6.9 g/dL
- May 20 PM7.2 g/dL
- May 21 AM7.1 g/dL — after transfusion. New IV required for retest.
- May 21 retest7.7 g/dL — required to meet discharge floor. Explanation from staff: “sometimes labs get bad samples.” Sometimes they get results for the wrong patient entirely. The patient absorbs every consequence of those errors regardless.
Normal range: 11.4–16.0 g/dL. Every number on that list is flagged low. Her hemoglobin dropped 1.7 points in 48 hours. Nobody asked why. The assumption: false positive on Monday. This has happened at least three other times since November — confirmed as false positives by licensed MDs on two of those occasions. One unit of blood raises hemoglobin approximately one point.
“Sometimes labs get bad samples.” The licensed providers — overworked, doing their best — are not responsible for bad samples. The patient who gets a new IV because of one, and waits another three hours while the system recalibrates around its own error — she absorbs that. Every time. Without acknowledgment.
“Her hemoglobin dropped 1.7 points in 48 hours. Nobody asked why.”

Thirteen hours. For a blood transfusion.
I want to take a moment to brag on Piedmont Henry Hospital. Melody needed blood. Her oncologist — a board-certified physician who has actually met her and everything — placed the order. And from that moment to the first drop of blood actually flowing: just 13 hours.
Thirteen hours. For a blood transfusion. For a dialysis patient with cancer. Who receives a transfusion — or two — every single week. Predictable. Scheduled. Known.
And they were so thorough. Three sets of labs. Two type and screens. Three room moves. You simply cannot cut corners like that and expect that kind of excellence. The new wing is going to be beautiful. They have Daisy awards. TULIP awards. The WiFi is tremendous. You’ll have plenty of time to enjoy it.
Plenty of time.
- 1:00 PMChecked in. “Fast tracked.”
- 6:00 PMStill in waiting room.
- 8:00 PMMoved to first room.
- 4:30 PMMoved to TCU unit.
- ~12:30 AMFinal move — observation unit. Large room, curtains, mandatory lights, enthusiastic staff who are clearly great friends. Wrong energy for midnight. Chorus of snores from other patients. Best. Date. Ever.
- ~1:00 AMBlood begins to flow. Approximately 12 hours after arrival. Transport was done by a nurse — unusual, usually a tech. She walked in and seemed genuinely surprised: “Did they already give you blood?” It appeared little had been communicated between shifts.
Why the delay? They needed to confirm she actually needed blood. The hemoglobin had shifted across the visit window — same false positive pattern, fourth instance since November. Instead of triggering a protocol review, it triggered more labs and more waiting.
They attempted a new type and screen. I spoke up. We had performed a type and screen that morning. In that facility. For that patient. For that provider. The response: “That one’s invalid. Protocol.”
“How long is a type and screen valid? Depends who you ask at the same hospital. Six hours. Twelve hours. Forty-eight hours. Seventy-two hours. Same hospital. Same patient. Same week.”
She is on oxygen — prescribed, documented, increased to 3 liters per hour by her physician. Every time they moved her, staff turned it back down to 2. Hospital protocol is 2. They rarely ask what the patient is actually prescribed. They just turn it down.
She had brought her own tank. The one the ED gave her had approximately one hour of oxygen in it. Seven hours passed before anyone connected her to hospital oxygen during a room transfer. Praise God she had the spare.
She has a documented anxiety diagnosis, treated with medication. Her blood pressure reached the 200s during the wait. The only medication available was a cardiac dose — administered three hours after the reading. Breathing treatments: not given. Standard morning medications: not given in full. In 24 hours, that is the complete medication list.
She checked in at 130s.
What you may not know about hospitals.
The hours between 6 and 8 — AM and PM — are dead zones for patient care. Paperwork. Shift change. If you are in the overflow ED unit, the one that doesn’t officially count as an admission, you are largely forgotten. There is a charge nurse on paper. In practice: minimum coverage, maximum gap.
Here is something worth knowing: hospitals are rated on ED admission rates. If the ED moves a patient to Observation — or to the overflow unit Melody was in — it does not count as an admission. When she returns for the same condition with the same outcome, it does not count against them with CMS. There is no one with full ownership of her care. No accountability trail.
“Her labs are fine.” If I hear those words one more time, I will be on the news.
The problem is not the people. I have watched nurses work impossible shifts with impossible ratios. And I watched one nurse sit with Melody for fifteen solid minutes when the transfusion finally started — monitoring, checking, doing exactly what protocol requires at the start of a blood transfusion. She was thorough. She was present. She was everything you want in a nurse at that moment.
That same nurse, those same protocols, seven hours earlier — and none of this happens. No 24 hour visit. No cascade. No two day recovery. The protocols exist. They work when they’re applied. The problem is the bureaucracy that delayed getting to that moment by half a day. It feels less like healthcare and more like HR policy. Corporate compliance dressed up in scrubs. And the people who bear the cost of that gap are not the ones writing the protocols.
The dangers of autistics watching processes.
We are both neurodivergent. I am AuDHD. Melody has anxiety and OCD. Both conditions are made measurably worse by prolonged stress, disrupted routine, and sensory overload. An ED — buzzing fluorescent lights, overheard conversations, full-volume speakerphone calls, constant movement, zero schedule — is the precise environment our brains process at full cost.
Research suggests neurodivergent individuals process up to 40% more sensory data than neurotypical people — some current studies cite higher. Up to. Not all. Not always. But the capacity is there, and under stress it compounds.
The work I had lined up that Monday — the client who came back after two missed deadlines, the auditions, the catching up — all of it stopped. At intake you never know for how long. The AuDHD project manager in me began sequencing immediately: what was due, what could move, what couldn’t, how many hours, what was cascading. I ran that loop for 24 hours on two hours of sleep.
What autistics do in environments like that — we watch. We track. We notice when the O2 gets turned down every single time without asking. We notice when the type and screen window changes depending on who you ask. We notice the patterns that polite people let slide because they don’t want to be difficult.
I am difficult. On purpose. Because she needs someone to be.
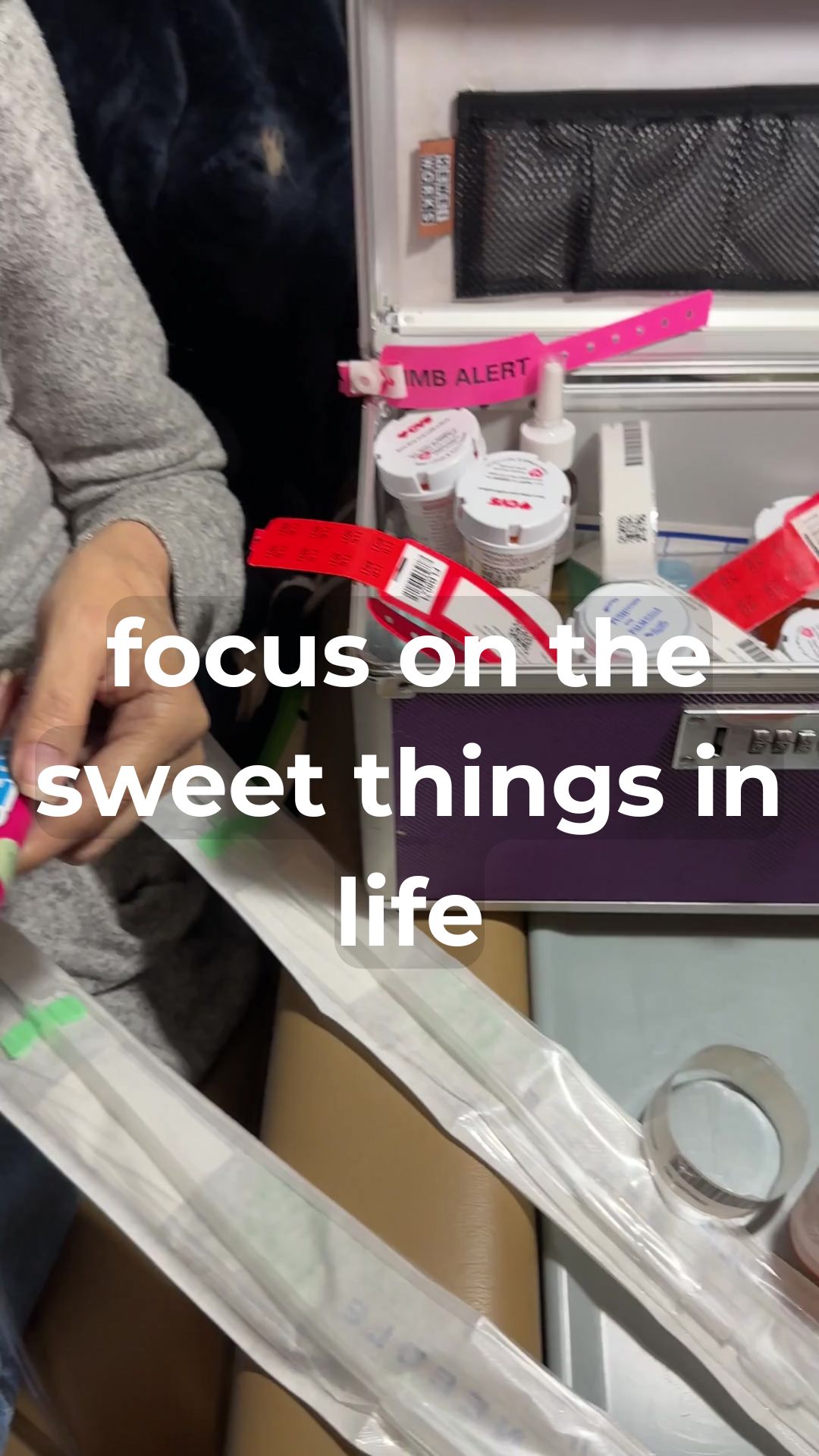
And then the blood began to flow.
It was past midnight. I had been awake for approximately 36 hours. She was in her third room. The folding chair had been my seat for most of the stay — not ideal for compressed lumbar discs, but here we are. Melody had not slept. Uncontrolled leg spasms, cramps, one episode of vomiting. The usual signs of low hemoglobin. The signs she had presented with since Monday. The signs they spent 12 hours confirming.
The transfusion took approximately four hours. The entire ED visit: just over 24.
I had posted that morning. Silly photo. Sunflower purse. Optimistic:
“Checking in for Medical Assistant duty! They need a cute one for tonight’s shift. My purse is super cute too — sunflowers, perfect match to my shoes. How does Melody get so lucky?”
— My post, the morning of the ED visit
Neither of us knew. That’s the part that stays with me.
One ripple. One week.
She was discharged exactly 24 hours after checking in. Thursday — dialysis day — she had nothing left. Skipped it. Friday: back to back to get back on schedule.
Her mother’s birthday celebration, postponed. Her counseling appointment, missed — the one she had that same Wednesday, already double-booked because of the extra labs. If anyone needs professional support right now, it is her. Ironic that it is Mental Health Awareness Month. I have some thoughts about mental health care access in Georgia. That is a blog for another Wednesday.
One ED visit that should have taken four hours took twenty-four. That one ripple cascaded into a missed birthday, a skipped dialysis, a back-to-back treatment, lost work days for both of us, and two days of recovery before either of us had functional bandwidth again.
“It’s just a blood transfusion. Should have been home by evening. That’s what we told her mother.”
Recovery. In our terms.
You and I might bounce back from a sleepless night in a day. For Melody — CKD, dialysis, MDS, hypertension, a worn-out vascular system — the toll compounds. Two days. Two quiet, calm days before anything resembling function returns. Not laziness. Biology.
For me, AuDHD recovery from 36 hours of sensory overload, schedule destruction, and sustained advocacy in a hostile environment looks similar. Two days where the bandwidth simply isn’t there. The sequencing that usually runs constantly in the background goes offline. The work waits. The emails wait. Everything waits.
That is the hidden cost no one accounts for. Not in the billing. Not in the discharge notes. Not in the CMS ratings. Two people. Four days of lost function. For a transfusion that takes four hours and could have been scheduled.
This week.
It is Wednesday. Labs are today. At least this week — so far — there is only one appointment and a blood transfusion coming sometime. Here goes nothing.
I knew that Sunday night, lying awake running the week’s calendar the way I always do. Two things I could account for. One lab appointment. Nothing else to cascade if things went sideways.
They have a way of going sideways.
This is Episode 1 of Wife Wednesday. The story continues every Wednesday. Follow on Instagram so you don’t miss it.
Follow the series. Every Wednesday — the unfiltered truth about caregiving, chronic illness, and a system that can do better. If this resonated, share it. Tag someone in healthcare. Tag someone who deserves better than this.
If you want to support Melody directly — parking, prescriptions, the things that add up quietly:
@thepaulspringfield on Instagram · paulspringfield.com · #WifeWednesday