The week that almost went as planned…
![[ Replace with hero image ]](http://paulspringfield.com/wp-content/uploads/2026/06/IMG_9797.mov)
The Week That Almost
Went as Planned.
Labs Monday. Transfusion Tuesday. Emma. A picnic of opposites. And next week is already loaded. This is Episode 2.
Sunday night. Running the calendar.
These days I eventually get to sleep around midnight or 1am, and usually awake by 4am — not up, but eventually I have no choice, and my day starts at 5. Despite the daily thoughts, something magically happens on Sunday nights. I thought it was maybe related to church — bearing the burdens on the hearts of our brothers and sisters has a cost — but we changed worship to every other week, so that wasn’t it. I tend to lean into my “insomnia is cool” aesthetic, and chief among those thoughts are the week ahead. What do I need to do, where, and by when. Constant thought, especially factoring in the expected ripples related to transfusions.
This week looked manageable. Almost a vacation week for medical engagements. Labs Monday, and a transfusion probably coming — the 6.8 was going to need addressing. That’s it. Nothing else to cascade. Let’s see how close to reality it is.
Monday morning. No doubt.
She started feeling a little energy over the weekend, so of course — welcome to Monday. She got up and there was no question. Labs confirmed what we already knew. How did we already know? She has trouble walking. Breathing is more difficult. General weakness in her legs, plus a particular pain. The body announces it before the labs do.
Surprisingly, the transfusion was scheduled for the next day. Which means: pack up. Wheelchair, oxygen tank and carrier, bag with creature comforts. Head to — not the infusion center, but the oncologist’s office first.
The infusion center requires a signed consent form — on paper — generated by the doctor’s office, in order to be permitted to dispense the life-saving blood. Every transfusion. The form that used to be signed once a year is now signed every single visit.
So the sequence is: roll her and an O2 tank to the doctor’s office, sign the form, sometimes conversation, then roll next door. They are in the same building — one half oncology, the other half infusion center. A small administrative detail, maybe.
Except nothing is small when four out of seven days she can barely walk across the room. Just about the time she recovers, feels the transfusion working, has a little energy — she’s back. The cycle resets before the benefit fully lands. That is what life with chronic illness looks like.
She has also been managing a nosebleed. Not dramatic. Persistent. The kind you work around because everything else doesn’t stop for it. Related to her conditions — and when every symptom’s advice is “go to the ED,” you can imagine she quietly manages it. Probably doesn’t help with platelets and hemoglobin either.
Meet Emma.
Emma recently joined the infusion center team. Thoughtful, curious, and as evidenced this week, totally willing to go well above and beyond.
Emma looked at the chart. Saw the labs. And as a practitioner, asked a question: why is the order for only one unit? We had that same discussion at our last oncology appointment, and again just minutes earlier when signing the consent form. The theory is that two units increases the risk of rejection and intolerance. The question now on the table — still open — is what the difference actually is between two units at once versus one unit twice a week in terms of cumulative risk, hemoglobin recovery, and quality of life between treatments. Emma was willing to take that question directly to the oncologist. That conversation is ongoing.
What matters is she asked. She didn’t just execute the order. She thought through the logistics — time needed, time to start, Melody’s preference for not starting early morning. That is a working practitioner. Not order-taking, not assembly line. Actually thinking like a medical provider, looking for ways to improve quality of life and outcomes.
That’s what it looks like when a clinician treats the patient instead of just executing the order.
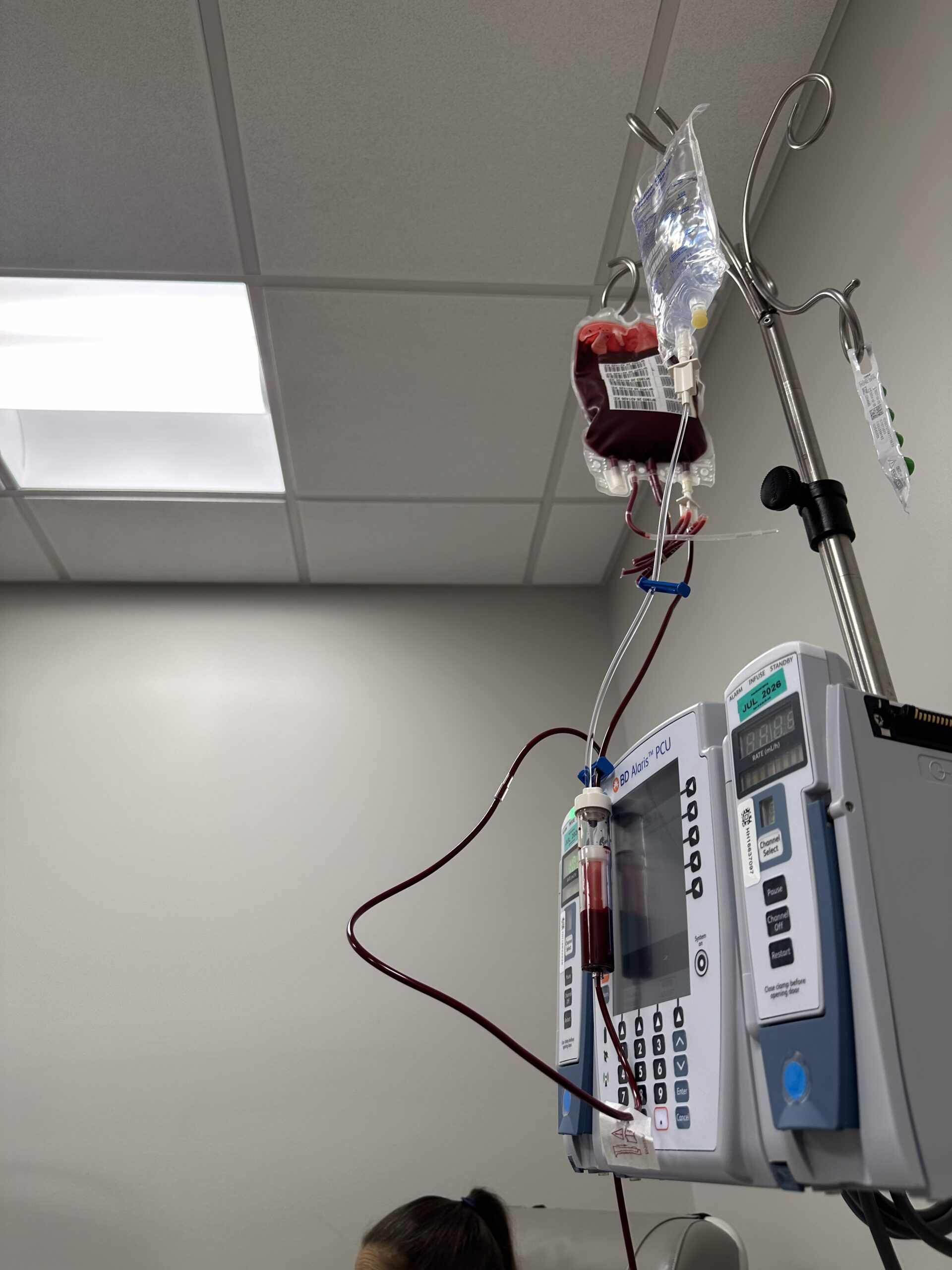
BP went down throughout the session. Not up. Down. Emma ran it cautiously, carefully, the way it should be run. If you read last week you know exactly why that sentence carries weight.
When Emma first joined the infusion team she noticed Melody needed a port. Asked the doctor. Procedure scheduled. We had noted it with the doctor, and the other nurses were aware of the blown veins and duplicate sticks. What a refreshing change. Here is the funnier part — remember the port issue in the ED last week? The port specifically for blood transfusions and chemotherapy, the procedure the ED told us they had no one certified to perform? Emma trains those nurses. At that ED. The issue was time and protocol. Not certification.
In her first weeks on the team, Emma noticed a port was needed and got it scheduled. She questioned a standing order based on the actual labs in front of her. She ran the transfusion the way it should be run. She opened a clinical conversation that hadn’t been had.
One person paying attention changed the arc of Melody’s care.
A picnic. Of opposites.
This week’s transfusion was a picnic in comparison to last week. Mild weather, sunshine, a gentle breeze, and Melody could feel the sunshine on her shoulders.
Bonus points if you can name that song.
You know that feeling when you’ve had a bad flu and you finally get one afternoon where you feel almost human? For Melody, that’s a good day. When she needs a transfusion she feels worse than that. The difference between last week and this week was not the disease. It was not the procedure. It was Emma. It was the rate. It was being treated like a patient instead of a unit of work.
Humanizing human patients leads to better outcomes. For the administrators and practitioners reading this — that was intentionally in your language.
There’s no such thing as a free transfusion.
Even when it goes right — and this one did — there’s a cost. On my end, AuDHD forced rest. Not chosen. The kind where the system finally stops because it has no choice. Three days of backlog waiting. The chores that don’t care what kind of week it was. Client deliverables that don’t either. Executive function just leaves — doesn’t even clock out.
And the ripple. Dialysis shifted. She was just too tired — two treatments this week instead of three. Same procedure, done right, still has a cost.
We will absolutely take the one that costs the least.
Imagine what last week’s version costs.
Same patient. Same procedure. Same week of the month.
One visit: 13 hours before the first drop of blood. 23 hours from the time we left home until we walked back through our door.
This visit: next day, BP down, Emma, right rate, sunshine on her shoulders.
The difference isn’t the disease. It’s the process. These are problems that don’t have to be problems.
Sunday night. Again.
It is Sunday night and I know what next week looks like on paper. Labs Monday. Medication management Tuesday — we found out Friday afternoon, great notice. Pulmonologist Thursday. Sleep study Saturday.
Sleep study means sleeping somewhere that isn’t home. With neurodivergence. Three days notice.
And a transfusion. We already know it’s coming. O2 tanks back to every location Monday. Emma let us take their O2 tank — they provide enough for the whole treatment, not just an hour’s worth like the ED. I wanted to get that back as soon as possible. I can’t expect professionalism from a provider if I’m not professional myself. And since I forgot the tanks when we exchanged ours, those needed to go back too — so that’s my Monday morning, on the way to labs.
This is what it looks like on paper.
Come back Wednesday to see how it actually went.
Follow the series. Every Wednesday — the unfiltered truth about caregiving, chronic illness, and a system that can do better. If this resonated, share it. Tag someone in healthcare. Tag someone who deserves better than this.
If you want to support Melody directly — parking, prescriptions, the things that add up quietly:
@thepaulspringfield on Instagram · paulspringfield.com · #WifeWednesday